Bed rest instead of continuous alarm
Beeping devices, humming machines, slamming doors, loud conversations: Noise sources in hospitals fight for attention, delay the healing of patients and promote mistakes in the operating room. The main culprits are continuous alarms, although almost 90 per cent of them do not require clinical intervention. In order to reduce the noise, scientists and sound designers are working on new concepts: continuous alarms are replaced by healing sounds and dissonance.
Acoustic environments, which can be classified as noise rather than harmony, are part of everyday life in hospitals. Besides light, air, work interruptions or precarious space conditions, noise is among the numerous systemic problems in healthcare buildings.
With peaks of up to 96 decibels, the noise in an intensive care unit is as loud as a high-traffic street. According to measurements, the continuous sound level ranges between 60 and 65 decibels (TU Graz 2013), and is thus ten to 50 decibels higher than the noise limit recommended by the World Health Organisation (WHO). According to the guidelines, an upper limit of 40 decibels during the day and 30 at night should not be exceeded in hospitals.
Above these levels, sleep disturbances and damage to the endocrine and cardiovascular systems may occur. Already at a noise level of 60 dB, EEG changes are noticeable among sleepers. The depth of sleep is reduced and a healthy person wakes up. This limit is also called the awakening threshold. In the case of old or sick people, this limit is already reached at 50 dB. Disturbed sleep can lead to stress. If sleep disturbances persist for a longer period of time, this can lead to a reduced response of the respiratory centre to the partial pressures of CO2 and O2, as well as to an exhaustion of the auxiliary respiratory muscles.
Critical noise levels
Several studies see a correlation between chronic noise and an increased risk of heart attacks. They found an increase of up to 50 percent, regardless of whether noise is subjectively perceived as annoying or not. No doubt about it: Continuous noise sets off a permanent alarm in the body. Adrenaline levels rise, blood pressure and blood lipid levels shoot up, making people more vulnerable to cardiovascular diseases. And there even seems to be a direct interaction between the auditory system and other areas of the central nervous system. Also cognitive disorders can be a consequence to noise exposure.
Particularly in the intensive care unit, high noise levels are harmful: weakened patients are flooded by the multitude of acoustic stimuli. With the simultaneous restriction of visual stimuli in the often windowless stations, this causes "enormous stress, often even states of confusion", describes Wolfgang Söllner, Director of the Clinic for Psychosomatics at Nuremberg Hospital. Cancer patients and patients in palliative care wards particularly suffer from the noise. Even sedoanalgesic patients perceive noise.
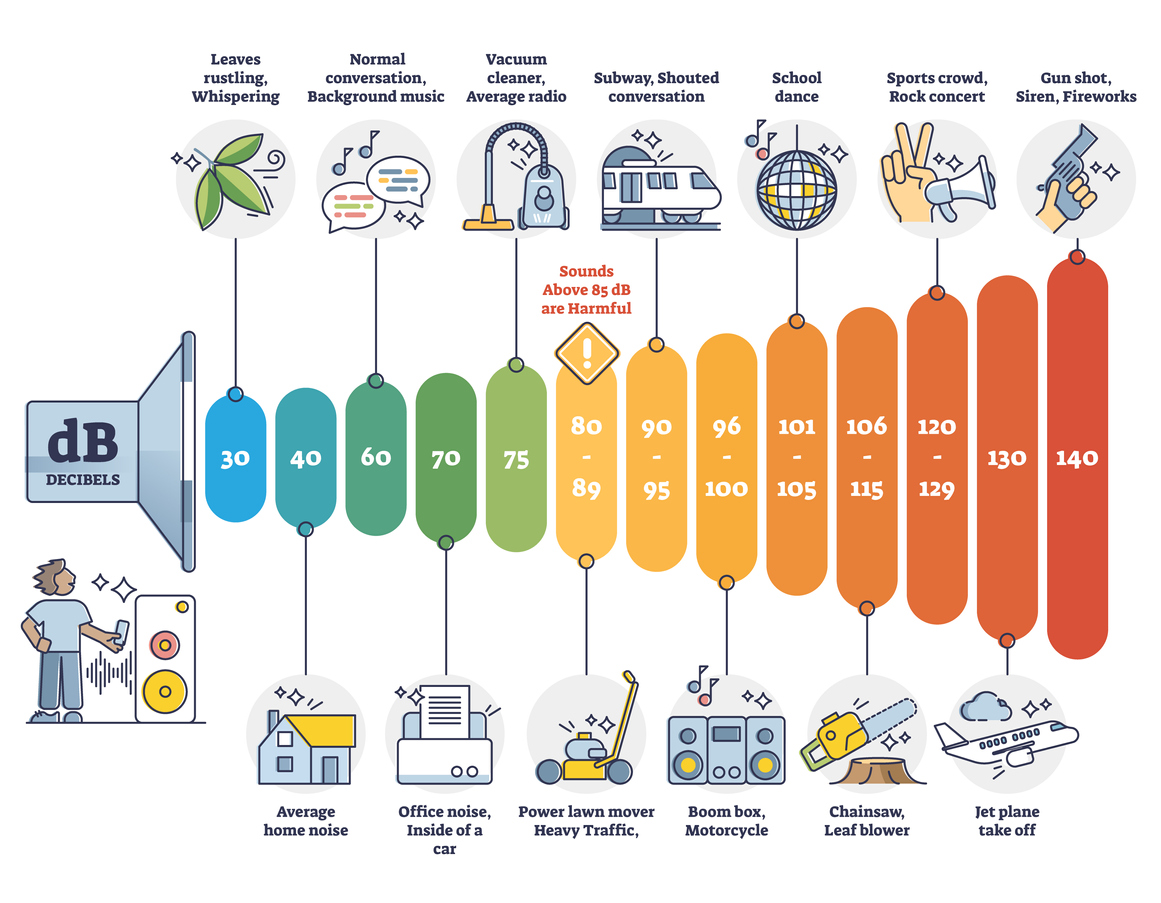
The hearing threshold lies at 0 decibels; at 30 dB and above, sleep disturbances can occur; at 50 dB and above, the ability to learn and concentrate decreases; at 65 dB and above, there is an increased risk of cardiovascular diseases; at 85 dB and above, hearing damage is possible with an exposure of 40 hours/week; at 120 decibels and above, hearing damage is possible after a brief period of time. Source: iStock
An army of noise
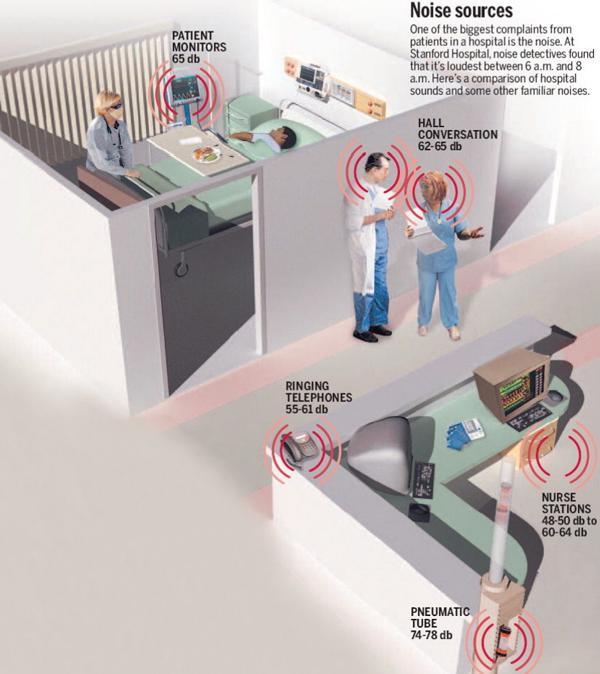
Scientists have been studying different sources of noise in hospitals for several years. They found that the most dominant noise pollution comes from staff conversations (35.4 per cent) (Landeskrankenhaus Villach 2014). A chat between four people, which often takes place during ward rounds, is around 74 decibels. Followed by monitor alarms (34.1 per cent). With at least 80 decibels, many alarms sound as loud as an argument or a passing car, and thus the limit that is defined as transition too loud.
Other noise disturbances include phone calls, ringing doorbells and slamming doors, which range at 86 decibels. Tearing open glove wrappers reaches a sound pressure level of 86 decibels, lowering a bed rail 90 and dropping a kidney dish 95 decibels. When the flap of a mobile X-ray machine closes, the sound reaches up to 92 decibels, when suction catheters are torn apart it hits 80 decibels, urine bottles clattering and cupboards slamming reach up to 76 decibels, or the noise of the secretion extractor exceeds 59 decibels and the dishwasher being emptied at up to 70 decibels. But while beeps and alarms can be irritating, a small study at the renowned John Hopkins University found that patients are most disturbed by the sounds of other patients. In particular, the voice of someone suffering from pain was mentioned.
In general, people perceive noises in the range between 40 and 65 decibels (dB) as being "normally" loud. However, our hearing can already be permanently damaged at a volume of 80 to 85 dB, says the German Professional Association of Ear, Nose and Throat Doctors.
Operating room and intensive care unit with the highest noise levels
Compared to other hospital areas, noise occurs more frequently and more severely in the intensive care unit. Meanwhile, the average volume of recorded ambient noise at night is 52.85 dB, with maximum values between 85.5 and 98.3 dB. Noise levels above 70 dB appear an average of ten times per hour. The recommended noise level is also regularly surpassed during the day. A similar picture is found at night, where staff discussions pose the main problem.
However, the highest noise levels were measured in operating rooms. Peak levels above 90 dB were the norm, but also levels above 105 dB were measured for at least ten percent of the time during operations in all clinical specialities, and therefore comparable to the volume of a chainsaw or a rock concert. Long-term sound measurements at John Hopkins Hospital showed values between 57 and 70.5 dB per operation, based on operation periods of 19 to 548 minutes.
Preventing complications for patients through silence
Exposure to high noise levels has devastating effects on medical and nursing staff as well. Medical staff become more prone to sickness and also increases the risk of mistakes. Verbal communication is limited by high noise levels. Monitoring equipment and treatment devices often beep and buzz in the same frequency range as human speech. This forces doctors and nurses to speak even louder, which in turn raises the general noise level.
The volume of the spoken word must be 15 dB above the background noise level to be heard. However, when the speech level rises by 10 dB, speech comprehensibility is reduced by 15 to 40 per cent due to the associated distortion of speech. From maximum levels of 55 dB(A), speech clarity is already affected; with further rise of the sound level, attention is reduced and the frequency of errors grows.
Doctors cannot focus well. And they might misunderstand each other, for example when giving orders during an operation or prescribing medication. Doctors in the operating rooms are required to maintain a high level of concentration, often for extended periods of time, and verbal communication is of the utmost importance in this setting. In 2006, a Swedish study on the effects of room acoustics found that noise-related stress was linked to emotional exhaustion and burn-out among intensive care physicians, which in turn threatenes patient safety.
Alarms are often unnoticed
And yet the permanent blaring of alarms, for example, is only necessary to a certain extent. Almost 90 per cent of alarms are false positives, hence false alarms can often lead to an interruption of work and to misconduct: Alarm limits are adjusted to critical ranges so that an alarm sounds less frequently, the volume is reduced so much that the alarm can be overheard, or ignored altogether.
The longer medical staff is exposed to continuous alarm sounds, the more time it takes to respond, and the risk of misinterpretation of warnings rises. This response time decreases because the stimuli are no longer perceived as a warning; this is known as alarm fatigue. Almost every two minutes, medical staff and patients are disturbed by acoustic alarms. The more patients there are on a station, the greater the intensity of the background noise. There are between 150 and 300 alarms per patient every day. Various studies show that each intensive care patient cause more than six alarms per hour. It is estimated that a doctor hears an average of 950 alarms per shift.
According to a study in the journal Critical Care(2001), medical staff respond to only one in ten alerts. A 2007 study found that after a device call, it sometimes takes up to 40 minutes for help to arrive. Alarms that are relevant to treatment go unnoticed, are ignored or even switched off in up to 50 percent of cases, assuming that it is a false alarm. Nursing staff often no longer react appropriately to the warning signals.
Noise levels rise, technification grows
And noise levels continue to rise: since the mid-20th century, levels have increased by about 20 decibels, a fourfold increase in noise intensity. Since 1960, daytime noise levels have risen from an average of 57 to 72 decibels (dB), according to a study by John Hopkins University. Nighttime noise levels in hospitals climbed from 42 to 60 dB over the same period.
There are many reasons for the increased noise pollution. For instance, the growing use of technology has increased the number of potential noise sources. But the increasing permissiveness in dealing with visiting rules also leads to an increase in ambient noise. " Hectic and noise span the entire day in some departments," says social medicine expert Stefan Willich. To protect other patients in need of quiet, he advocates setting up separate visiting rooms for visitors.
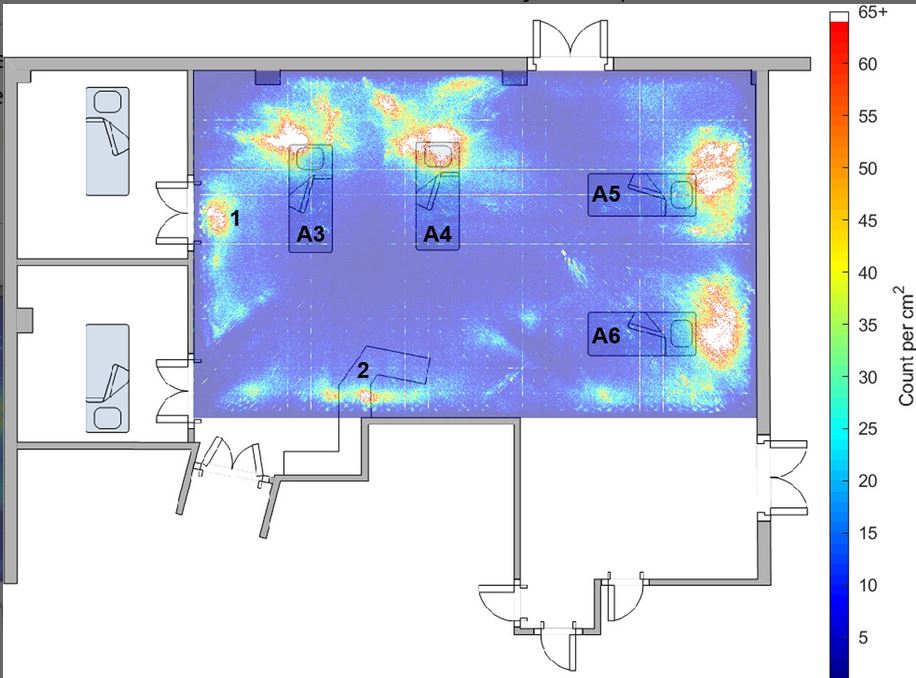
This graph can be interpreted as an average "noise map" for an intensive care unit. The "hotter" colours (red and yellow) indicate areas where loud noises were more frequent.
Connecting devices
To solve this problem, experts suggest developing alarm systems that take environmental factors into account. An ECG monitor for heart rate, for example, could be coupled with sensors that measure whether the patient is moving. In that case, an accelerated pulse could be attributed to a harmless muscle tremor, for example - and would therefore not be a reason for a medical alert. Another way to achieve fewer alarms while maintaining the same sensitivity would be to connect the existing devices with each other. This would allow a clear overall picture to be created from the multitude of measured values. However, since hospitals often use systems from very different manufacturers, this would not be easy to implement.
Networking is also a legal problem. "At the moment when, for example, medical devices are integrated into an IT network and communicate with this network, the responsibility for correct communication lies with the owner If a vital alarm fails to sound due to a programming error, the hospital would consequently be liable and not the equipment manufacturer.
Even minor technical and organisational changes could reduce the sound level in many places, says Professor Stefan Willich, Director of the Institute for Social Medicine at the Charité in Berlin. He mentions the alarm devices in intensive care units as such an example: "Why does the patient have to hear the beeps? They could be directed to the outside." Changing the acoustic monitor alarms to vibration or visual signals could reduce noise pollution.
"Bathroom" acoustics
In addition to noise sources such as alarms and conversations, there are other indirect sources of noise such as walls, floors and ceilings, most of which are sound-reflective rather than sound-absorbent. This is known as the problem of bathroom acoustics. In hospitals, one cannot put carpets on the floors, nor can one put porous material on the ceiling, because bacteria can get in there and risk the necessary hygienic conditions.
This was the problem that acoustic engineer James West looked at. He redesigned a children's clinic at John Hopkins Hospital and hung large sheets of sound-absorbing material under the hospital's ceilings. He used fibreglass-reinforced plastic commonly used for thermal isolation as sound insulation. Since it is not washable, it was packed in a sort of rubbish bag. For this, West found a special material that is suitable for a germ-free environment. It can be taken down and cleaned. The redesign had an effect: the equipment halved the so-called reverberation time, which is the time it takes for a sound to fade away.
"Healing Architecture and Silent Hospitals
An increasing number of hospitals are testing noise-reducing measures, such as noise lights or soundear systems. The devices measure the volume and warn of excessive noise levels with pictograms or traffic light colours. Others rely on noise-cancelling headphones for patients. This system was originally designed to filter out ambient noise from the listening experience of music lovers.
Another concept for noise reduction are the so-called "Adaptive Healing Rooms". The newly designed intensive care rooms, which are already in use at Münster University Hospital and Berlin's Charité hospital, have an intelligent alarm system that prevents unnecessary noise. Medical equipment largely disappears behind wall panelling and a lighting control system simulates sunlight to achieve an improved day-night rhythm for patients. It is assumed that such patient rooms will only be reserved for privately insured patients and will not be affordable for every hospital due to cost-intensive conversions. In the meantime, "healing architecture" has developed into its own branch of research.
Raising staff awareness
However, it can be done without spending financial resources, as the project hospitals in America known as "silent hospitals help healing" show. One project was launched at Montefiore Medical Center under the name Silent Hospitals Help Healing (SHHH). Here, various measures were taken to make the hospitals quieter. For example, transport trolleys were repaired and telephones were changed to vibrate. Staff shift transfers have become quieter and visitors are encouraged to talk more quietly. There are stickers on the doors, with a nurse holding a finger to her lips, asking for more silence. These measures have led to a reduction in noise levels from a measured 78 decibels to levels between 50 and 60 decibels. Initial effects have been that patients sleep significantly better and staff are less stressed.
Other steps taken to reduce noise include soft soles on staff shoes and a reduction in the volume of the public speaking system. Staff training is thus a cost-effective way to improve the noise situation in intensive care units. A study by the Hanover Medical School also shows that raising staff awareness can be effective. After staff members were trained on how to avoid noise in the operating theatre, for example by talking less and switching off telephones, the noise intensity finally dropped to half of the original value in the third phase of the study - with the result that the staff in the operating theatre is measurably better off because they can work in a quieter environment. This was also verified by the stress hormones in the saliva, skin resistance and the questioned subjective feeling. The well-being of the patients also improved and there were up to 50 per cent fewer complications during operations.
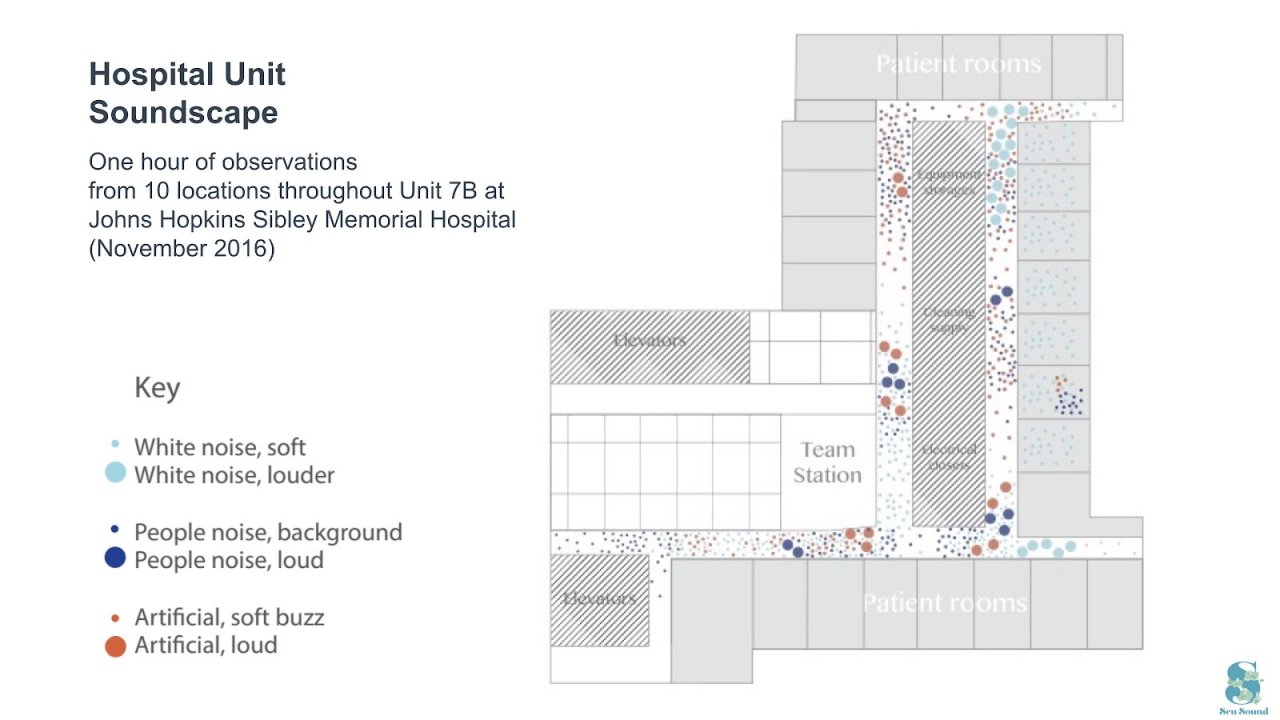
This graphic shows the background noise at John Hopkins Hospital. Dark blue dots represent conversations.
Newly composed soundscape
Another possibility is to cover the noise with other sounds. The use of white noise, for example, is recommended as a method of masking ambient noise, improving sleep and maintaining sleep in the coronary care unit. Sound designers and musicians have also tackled the problem. Japanese musician Yoko Sen has been working with scientists, patients, caregivers and equipment manufacturers on various concepts to replace shrill alarm systems with more soothing sounds for several years. Sen, who mainly composes electronic music, started her project SenSound in 2015. You can hear an audio example in this video clip. An important aspect of this is to harmonise the individual sounds of the monitoring devices. Rather than risking to confuse the staff by radically changing the alarms overnight, she recommends simply changing the alarms. overnight, she recommends simple adjustments, such as slightly changing the pitch of an alarm. Sen also designed a "Tranquility Room", a space that relaxes with soothing sounds, dim lighting and aromatherapy to help patients relax. Judy Edworthy went one step further. The psychologist has been involved in the development of medical alarm systems for decades. In July, the International Standards Organisation approved a new set of alarm designs created by Edworthy that simulate the natural hospital environment. Health Canada-approved standards include an electronic heartbeat sound for alarms related to heart problems and a rattling pillbox for medication administration. Edworthy says these new alarms can be more easily identified and located by nurses and doctors, while improving the overall ambience of the hospital.
Different sounds for different parameters
Scientists at the Delft University of Technology in the Netherlands are working on a different approach with their Critical Alarms Lab. For years, scientists there have been researching patient- and staff-friendly noisescapes for intensive care units. In their "Caretunes" concept, alarms are to be replaced by disharmonies. For example, the heartbeat, the oxygen level and the blood pressure form a harmonic melody. A bass is heard for the heartbeat, a guitar chord for the oxygen content and the blood pressure is symbolised by a bell. If one of the components sinks or rises, the pitch changes in each case. Through the now created and noticeable disharmony, it is supposed to be recognised that the condition of the person concerned has changed. Markus Redmann, ward manager of the intensive care unit of a Cologne hospital, can appreciate the approach that different parameters have different tones. In general, he says, alarms are often too unspecific, they are switched in such a way that staff hear that something is wrong but have no idea what the exact problem is.
Recommendations of Heidelberg University Hospital and Montefiore Medical Center to minimize noise
- Nursing and medical interventions, if they are routine procedures, should be avoided during the night
- Sleep and sedative medications should not be the only means of treating sleep disorders, but always serve only as support
- Occupation during the day (mobilisation, cognitive occupation, basal stimulation) fosters tiredness, falling and staying asleep.
- All members of the interdisciplinary team (doctors, nurses, physiotherapists, etc.) are to contribute to a good night's sleep for intensive care patients.
- The doors to the patients' rooms should be closed or left slightly open at night
- Reduce light in patients' rooms, e.g. by using darkened modes on the ventilator
- Reduce noise, e.g. by reducing the volume of alarm signals and avoiding private conversations at the patient's bedside
- Opening packages makes a lot of noise; activities like this can also be moved to the corridor.
- Patients who are being gradually withdrawn from artificial respiration ('weaning') should be allowed to recover at night. Pressure-controlled ventilation is preferable to pressure-supported ventilation.
- A thorough anamnesis at the beginning of treatment with the support of the relatives helps to identify personal preferences (special sleeping habits etc.) of the patient in advance.
- Hold prolonged meetings in the common room or staff base
- If possible, do not carry out administrative tasks, work on the computer or make appointments by telephone in the patient's room.
- Work shoes should be designed with quiet soles. (Montefiore Medical Center 2008)
- Placing signs on the premises to encourage quiet behaviour, is one way of reminding both visitors and staff to behave quietly. (Montefiore Medical Center 2008)